2019 E-Consult Workshop Recap
The fifth annual E-Consult Workshop, held November 4, 2019, featured presentations on the “E-Consult Journey” to address e-consult adoption, policy, regulation and payment. The Workshop included discussion of recent DHCS reimbursement changes and upcoming Medi-Cal waiver renewals that could impact e-consults’ acceptance by consumers and payers and its use by providers. Below are summaries and links to these presentations.
View E-Consult Workshop presentations slides.
Keynote Speakers: E-Consult Journey
- Delphine Tuot, MD, Associate Professor, Nephrology, Zuckerberg, San Francisco General, Associate CMO of Specialty Care and Diagnostics
- Douglas Archibald, PhD, Assistant Professor and Educational Research Scientist, Department of Family Medicine, University of Ottawa
- Paul Giboney, MD, Associate CMO, Los Angeles County Department of Health Services
Payer Strategies for E-Consult
- Tanya Dansky, MD, VP & CMO, Blue Shield Promise Health Plan
- Joel Gray, Executive Director, Anthem Blue Cross
- Somer Harris, Telehealth Program Manager, Partnership Health Plan
- Sajid Ahmed, CEO, WISE Health Care, Consultant to Inland Empire Health Plan
What Challenges Remain
- “Engagement and Scale”, Mark Schweyer, Director of Telehealth Programs, Health Net
- “Operationalizing”, Daren Anderson, MD, Director of Weitzman Institute, VP/CQO of Community Health Center, Inc.
- “Payment”, Mike Witte, MD, Vice President and CMO, California Primary Care Association
- “FQHC Programs”, Ella Schwartz, Director of Operations, Community Health Center Network
State Policy Perspectives
- Paul Giboney, MD, Associate CMO, Los Angeles County Department of Health Services, and David Lown, MD, CMO, California Health Care Safety Net Institute
- Dan Southard, Deputy Director, Office of Plan Monitoring, CA Department of Managed Health Care
Delphine Tuot, MD, UCSF, Zuckerberg, San Francisco General
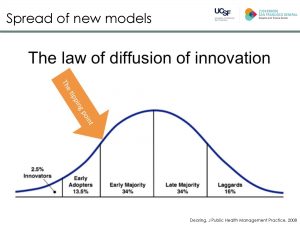
Kicking off the day, Dr. Tuot explained how improved patient satisfaction, provider experience, and population health, along with lower costs, have spurred adoption and moved e-consults past the Innovator and Early Adopter phases on the curve of innovation diffusion. “This tipping point is where I think we are in our e-consult work, and the question is how do we push it up to the curve,” stated Dr. Tuot. In order to increase e-consult adoption, early adopters still need to report and share program data, she added. View presentation.
Douglas Archibald, PhD, University of Ottawa
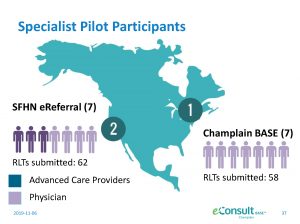
In 2011, the University of Ottawa broke e-consult ground in Canada and since then it has been at the e-consult forefront pushing its innovation and adoption across the country. In 2018, the number of e-consults completed by the Champlain Base program exceeded the total it delivered over the five year period between 2011 and 2015, explained Archibald. Archibald presented a summary of a new collaborative study among U.S. and Canadian researchers focused on the learning and teaching that goes on during the e-consult process “to show how e-consult learning may become part of certification and maintenance programs for providers.” View presentation.
 Paul Giboney, MD, Associate CMO, Los Angeles County Department of Health Services
Paul Giboney, MD, Associate CMO, Los Angeles County Department of Health Services
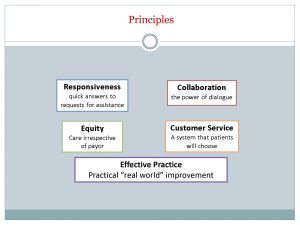
As a primary care provider and clinicals leader of LA DHS, Dr. Giboney has years of experience both working with e-consults and educating DHCS providers on its benefits and use. Between the LADHS e-consult launch in 2012 and 2019, 16,000 providers have completed over one million e-consults. To reflect upon the LADHS e-consult journey, Dr. Giboney presented five key e-consult adoption principles.
- Customer Service: The most powerful principle for telling the story of e-consult is the Customer Service, which is patient-centered care. For specialists, e-consults powerfullly eliminate “wasted time with low-value visits.”
- Collaboration: Two clinicians discussing a unique individual’s case is the height of precision or personalized medicine. Through e-consult connections, PCPs and specialists develop relationships that benefit patients.
- Responsiveness: With e-consult, we’ve taken an unresponsive system and turned it around into a responsive system. And we’ve been able to schedule patients for the right timeliness for their conditions.
- Equity: E-consults are blind to payer source. The specialists don’t see if they are discussing an uninsured patient, a Medicaid patient or a Medicare patient. They just see the patient and they respond according to clinical need.
- Effective Practice: E-Consult…broke the mold. By actually disrupting and innovating care delivery, e-consult really changed the way our system saw their ability to improve care.
Panel: Payer Strategies for E-Consult Program Engagement
The Workshop featured a panel of innovative payers who promote e-consult use among providers to ensure appropriate specialty care access for their members. Provider engagement examples included the following:
Sajid Ahmed, Inland Empire Health Plan “Like LADHS, IEHP has mandated e-consult, and since we launched in March 2018, our average number of e-consults is 5,000 a month. A key component of the program is that e-consult is mandatory.”
Joel Gray, Anthem Blue Cross “We are working to understand FQHC start-up costs and supporting them through grants. We are also launching a new PMPM incentive program toward HEDIS and quality measures for clinics. Clinics have a choice to use the PMPM earnings to support the additional time primary care providers need to manage a case.”
Somer Harris, Partnership Health Plan “To make the process easier for PCPs, we opened up our e-consult platform to allow coordinators or clinical staff to submit e-consults on PCPs behalf. We incentivized the process so that the more consults a clinic submits the more grant funding they receive from the plan.”
Tanya Dansky, MD, Blue Shield Promise Health Plan “We have the great fortune to be able to run two clinics, so we are both health plan and ‘doctor’. We’ve done about 1,500 consults thus far for our health plan, and the satisfier for the PCP is that e-consult is just a button click.”
“Remaining Challenges”, Mark Schweyer, Health Net

“Health plans have become partners…and we need to determine how to have shared visions, goals and outcomes…At Health Net we have developed a program where we cover implementation and invest in payment for e-consults that are delivered on the primary care side because we recognize that’s where the lion’s share of the work is done.” View presentation.
“Operationalizing eConsults”, Daren Anderson, MD, Weitzman Institute
“We have to start talking about cost savings, efficiency and patient experience as the reasons why e-consults are important…[And we should] make the process easy with features such as keeping the PCP in their own EHR, capitalizing on existing workflow, and using coordination staff to submit the e-consults.”
“eConsult…and…Payment Reform?” Mike Witte, California Primary Care Association
“We need to take a look at what is the real value of e-consults…We can define e-consults as a conversation that has value in it that leads to better outcomes at decreased costs.” View presentation.
“Electronic Consults and FQHCs,” Ella Schwartz, Community Health Center Network, Director of Operations
“Overall, our e-consult program represents just 1% of what we spend on specialty care…We’ve spent the last few years trying to change PCPs use of e-consults by training them on the program’s qualitative and quantitative value. And now we are having the same conversations with our local specialists…We have great program and we’re working to determine how to make it seamless and beneficial for both PCPs and local specialists.” View presentation.
“PRIME, QIP & GPP: Current and Future” Paul Giboney, MD, Los Angeles County Department of Health Services and David Lown, MD, California Health Care Safety Net Institute
 State funding for public hospitals is set to change in 2020. With the sunset of the PRIME (Public Hospital Redesign and Incentives in Medi-Cal) program in June 2020, California’s hospital pay-for-performance program will become the QIP (Quality Incentive Program) and include new measures starting in January 2021 that may reflect the use of telehealth and e-consult.
State funding for public hospitals is set to change in 2020. With the sunset of the PRIME (Public Hospital Redesign and Incentives in Medi-Cal) program in June 2020, California’s hospital pay-for-performance program will become the QIP (Quality Incentive Program) and include new measures starting in January 2021 that may reflect the use of telehealth and e-consult.
Today, hospitals use e-consults to meet PRIME goals. In the future, a measure may not mention e-consult specifically, but may allow e-consult to be incorporated into its structure. It will still be possible for providers to accrue points to capture GPP (Global Payment Program) funds using e-consult services for uninsured patients. These programs are looking for ways to help hospital systems build the competencies and capabilities to be high performing and deliver value going forward.
Dan Southard, CA Department of Managed Health Care (DMHC)
Southard explained that DMHC is in process of defining how to assess and give credit for telehealth use. He encouraged managed care plans to share their telehealth programs with DMHC and DHCS to increase the agencies’ understanding of e-consult and telehealth’s potential to increase access to care.